

A COURIOUS CASE OF COVID-19 GRAPHENE POISONING

Here is a very comprehensive, scientific article on the toxicity of GRAPHENE.
https://particleandfibretoxicology.biomedcentral.com/articles/10.1186/s12989-016-0168-y Toxicity of graphene-family nanoparticles: a general review of the origins and mechanisms

I looked at the toxicity of GFNs (Graphene family nanomaterials) in various organs or systems in animals and compared it with existing studies on C-19 complications and side effects of Covid-19 injections.
It is not perfect (the list, highlighted in pink, is not very comprehensive; there are so many other studies on these adverse effects), but nevertheless it clearly shows that literally ALL COVID-19 symptoms, as well as vaccine adverse effects, are identical to complications caused by GRAPHEN TOXICITY.
Since we know that graphene has been used extensively in this "pandemic," it should be logical to first see if it could be responsible for the bizarre (for a respiratory virus) symptoms and complications.
No literature I know of published until 2019, and I've read thousands of scientific articles, has proposed such a reckless use of graphene as a "miracle antivirus agent" on such an unprecedented scale - without considering its dangers.
Suddenly, graphene has been used in masks, in tests, in filters in respirators, in medicines, as a biocide to be sprayed in the air, and even in food and municipal water filters....
This is absolutely unprecedented, given the well-known toxicity and hazards associated with nanotechnology.
I postulate that we are facing a pandemic of poisoning the world's population with nanotechnology.
https://particleandfibretoxicology.biomedcentral.com/articles/10.1186/s12989-016-0168-y Toxicity of graphene-family nanoparticles: a general review of the origins and mechanisms | Particle and Fibre Toxicology |
Toxicity of GFNs (GFNs: Graphene family nanomaterials) in organs
The toxicity and biocompatibility of GFNs has been observed and assessed through theoretical and animal model studies. At present, there are a mass of data demonstrating the toxicity of GFNs (Graphene family nanomaterials) in different organs or systems in animals, so that it is hard to list all the data in this review. Thus, we summarized a certain number literature and chose some in vivo toxicological studies of GFNs listed in Table 1
Table 1 Toxicity of GFNs in organs
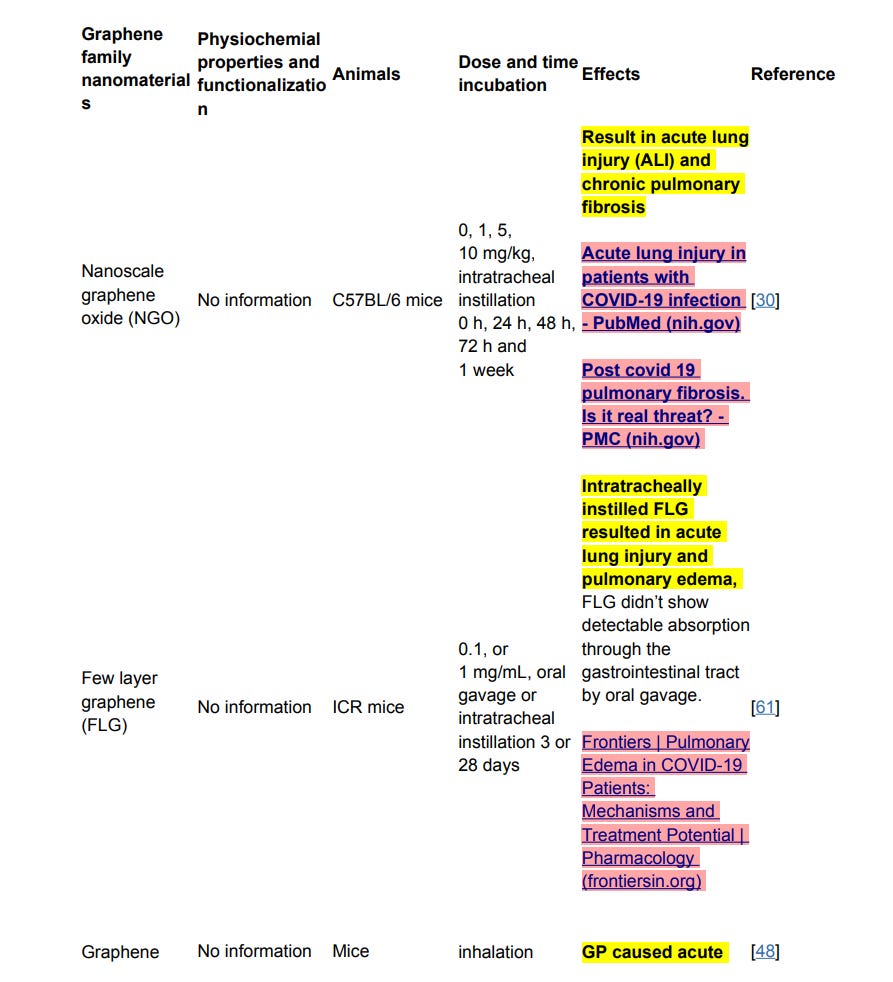






This review collects studies on the toxic effects of GFNs in several organs and cell models. We also point out that various factors determine the toxicity of GFNs including the lateral size, surface structure, functionalization, charge, impurities, aggregations, and corona effect ect. In addition, several typical mechanisms underlying GFN toxicity have been revealed, for instance, physical destruction, oxidative stress, DNA damage, inflammatory response, apoptosis, autophagy, and necrosis.
For Covid patients: https://www.sciencedirect.com/science/article/pii/S0006349521004549 Physical phenotype of blood cells is altered in COVID-19 Although the pathology is not yet fully understood, hyperinflammatory response and coagulation disorders leading to congestions of microvessels are considered to be key drivers of the still-increasing death toll. Until now, physical changes of blood cells have not been considered to play a role in COVID-19 related vascular occlusion and organ damage. Here, we report an evaluation of multiple physical parameters including the mechanical features of five frequent blood cell types, namely erythrocytes, lymphocytes, monocytes, neutrophils, and eosinophils. More than four million blood cells of 17 COVID-19 patients at different levels of severity, 24 volunteers free from infectious or inflammatory diseases, and 14 recovered COVID-19 patients were analyzed. We found significant changes in lymphocyte stiffness, monocyte size, neutrophil size and deformability, and heterogeneity of erythrocyte deformation and size.
https://www.sciencedirect.com/science/article/pii/S000296292100063X DNA and RNA Oxidative Damage and Mortality of Patients With COVID-19 - ScienceDirect What we know about COVID-19 and the inflammatory response (drugtargetreview.com) Observational studies of COVID-19 patients that required intensive care show higher than normal levels of the pro-inflammatory factors IL-2, IL-7, IL-10, granulocyte colony-stimulating factor (G-CSF), IP-10, MCP1, macrophage inflammatory protein 1α (MIP1α) and tumour necrosis factor (TNF)11 in their blood plasma. Clinical observations revealed that IL-6 was higher in non-survivors compared to those that managed to recover.4 Furthermore, high levels of cytokines like TNF are associated with septic shock and multiple organ failure, leading scientists to hypothesise this could also be causing myocardial damage and circulatory failure seen in some COVID-19 patients.4
https://www.karger.com/Article/FullText/513198 Hyperinflammation and Immune Response Generation in COVID-19 - Full Text - Neuroimmunomodulation 2020, Vol. 27, No. 2 - Karger Publishers The inflammatory response generated after infection by increased proinflammatory cytokines and chemokines, and complement proteins activation may likely contribute to disease severity,
https://www.frontiersin.org/articles/10.3389/fphys.2020.611275/full Modulation of Autophagy by SARS-CoV-2: A Potential Threat for Cardiovascular System
Along with the application and production of GFNs (Graphene family nanomaterials) increasing, the risk of unintentional occupational or environmental exposure to GFNs is increasing [26]. And recently, there are some investigations on GFNs exposure in occupational settings and published data showed that the occupational exposure of GFNs had potential toxicity to the workers and researchers [27–29]. GFNs can be delivered into bodies by intratracheal instillation [30], oral administration [31], intravenous injection [32], intraperitoneal injection [33] and subcutaneous injection [34]. GFNs can induce acute and chronic injuries in tissues by penetrating through the blood-air barrier, blood-testis barrier, blood-brain barrier, and blood-placenta barrier etc. and accumulating in the lung, liver, and spleen etc.
For Covid patients: https://www.nature.com/articles/s41422-021-00523-8?proof=tr A cohort autopsy study defines COVID-19 systemic pathogenesis In patients with systemic viral distribution, SARS-CoV-2 was detected in monocytes, macrophages, and vascular endothelia at blood–air barrier, blood–testis barrier, and filtration barrier. Critically ill patients with long disease duration showed decreased pulmonary cell proliferation, reduced viral RNA, and marked fibrosis in the lungs. Permanent SARS-CoV-2 presence and tissue injuries in the lungs and extrapulmonary organs suggest direct viral invasion as a mechanism of pathogenicity in critically ill patients. SARS-CoV-2 may hijack monocytes, macrophages, and vascular endothelia at physiological barriers as the ports of entry for systemic dissemination.
https://pubmed.ncbi.nlm.nih.gov/34232823/ The blood-gas barrier in COVID-19: an overview of the effects of SARS-CoV-2 infection on the alveolar epithelial and endothelial cells of the lung
https://www.karger.com/Article/Fulltext/509644 Splenic Abscess: An Unusual Presentation of COVID-19? Computed tomography (CT) abdomen showed the presence of splenic abscess and small intraperitoneal gas indicating pneumoperitoneum. Laparotomy revealed ruptured splenic abscess and splenectomy was done. The patient continued to show features of severe sepsis with multiorgan failure and died on postoperative day 16. COVID-19 mainly affects the respiratory system but extrapulmonary affection has been reported. Direct invasion and damage to the organs by the virus could be the reason behind the development of the extrapulmonary manifestations.
For example, some graphene nanomaterials aerosols can be inhaled and substantial deposition in the respiratory tract, and they can easily penetrate through the tracheobronchial airways and then transit down to the lower lung airways, resulting in the subsequent formation of granulomas, lung fibrosis and adverse health effects to exposed persons.
For Covid patients: https://onlinelibrary.wiley.com/doi/10.1111/ijcp.14110 The effect of COVID‐19 on lower urinary tract symptoms in elderly men We aimed to evaluate the change in lower urinary tract symptoms (LUTS) after COVID-19 in men LUTS may be one of the symptoms of COVID-19 in some patients. Elderly patients with increased LUTS should be evaluated for COVID-19 when the reason unclear.
The inhaled GO (Graphene Oxide) nanosheets can destroy the ultrastructure and biophysical properties of pulmonary surfactant (PS) film, which is the first line of host defense, and emerge their potential toxicity [54]. The agglomerated or dispersed particles deposit on the inner alveolar surface within the alveoli and then be engulfed by alveolar macrophages (AMs) [55].
For Covid patients: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8276044/ The Role of Pulmonary Surfactants in the Treatment of Acute Respiratory Distress Syndrome in COVID-19 The SARS-CoV-2 virus damages the AT-II cells and results in decreased production of PS. (…) SARS-CoV-2 enters the body through lungs via binding of viral spike protein with angiotensin converting enzyme 2 (ACE-2) receptor (Mason, 2020). After entry, SARS-CoV-2 is postulated to destroy type II alveolar cells, the site for the synthesis of pulmonary surfactants, resulting in decreased production of pS. Decreased surfactant production causes atelectasis and reduced the pulmonary compliance. The patients with Coronavirus disease 2019 (COVID-19) are presented with clinical symptoms which are very similar to those observed in NRDS (Nieman et al., 2018; Schousboe et al., 2020) for which deficiency in PS is the primary cause (Figure 2).
Blood-placenta barrier The placental barrier is indispensable in maintaining pregnancy, as it mediates the exchange of nutrients and metabolic waste products, exerts vital metabolic functions and secretes hormones [67]. A recent review suggested that the placenta does not provide a tight barrier against the transfer of nanoparticles to fetuses, specifically against the distribution of carbonaceous nanoparticles to and in the fetus [42]. It was suggested that rGO (reduced Graphene Oxide) and gold particles (diameter of 13 nm) are barely present or are absent in the placenta and fetus in late gestation after intravenous injection [44, 68]. However, other reports showed that transplacental transfer does occur in late gestational stages [69, 70]. Much attention had been paid to the developmental toxicity of nanomaterials, and reports showed that many nanoparticles did cross the placental barrier and strongly influenced the development of embryos [71–75].
For Covid patients: https://www.frontiersin.org/articles/10.3389/fimmu.2021.743022/full Frontiers | The Effects of COVID-19 on the Placenta During Pregnancy The majority of newborns delivered from SARS-CoV-2 positive mothers test negative following delivery, suggesting that there are protective mechanisms within the placenta. There appears to be a higher incidence of pregnancy-related complications in SARS-CoV-2 positive mothers, such as miscarriage, restricted fetal growth, or still-birth.
Current data demonstrates that GO (Graphene Oxide) sheets interact with the plasma membrane and are phagocytosed by macrophages. Three major receptors on macrophages take part in the phagocytosis of GNS: the Fcg receptor (FcgR), mannose receptor (MR), and complement receptor (CR). Furthermore, FcgR is a key receptor in the mediated phagocytic pathway [90, 93, 94]. The protein corona of GO promotes the recognition by macrophage receptors, especially the IgG contained within the protein corona. Macrophages were observed to undergo prodigious morphological changes upon contact with GO [34]. After internalization, graphene accumulated in the cell cytoplasm, perinuclear space, and nucleus, which induced cytotoxicity in murine macrophages by increasing intracellular ROS through depletion of the mitochondrial membrane potential and by triggering apoptosis through activation of the mitochondrial pathway [83].
For COVID-19 patients: https://www.sciencedirect.com/science/article/pii/S0014299920306397?via%3Dihub Macrophage responses associated with COVID-19: A pharmacological perspective A particularly insidious aspect of COVID-19 is the delayed overactivation of the body's immune system that is manifested as the cytokine storm. This unbridled production of pro-inflammatory cytokines and chemokines can directly or indirectly cause massive organ damage and failure. Systemic vascular endothelial inflammation and thrombocytopenia are potential consequences as well. In the case of COVID-19, the cytokine storm often fits the pattern of the macrophage activation syndrome with lymphocytopenia. The basis for the imbalance between the innate and adaptive immune systems is not clearly defined, but highlights the effect of SARS-CoV-2 on macrophages.
Toxicity in internal organs GO Graphene Oxide) can result in acute inflammation response and chronic injury by interfering with the normal physiological functions of important organs.
For COVID-19 patients: https://www.nature.com/articles/s41581-021-00452-0 Pathophysiology of COVID-19-associated acute kidney injury, https://pubs.rsna.org/doi/full/10.1148/radiol.2021211087 Detecting COVID-19–related Chronic Pulmonary Injury with 129Xe MRI, https://www.tctmd.com/news/both-acute-and-chronic-myocardial-injury-covid-19-impede-6-month-survival Both Acute and Chronic Myocardial Injury in COVID-19 Impede 6-Month Survival
A high dose of GO (Graphene Oxide) that forms aggregations can block pulmonary blood vessels and result in dyspnea [50, 98], and platelet thrombi were observed at high concentrations of 1 and 2 mg/kg body weight via intravenous injection [89].
For COVID-19 patients: https://jhoonline.biomedcentral.com/articles/10.1186/s13045-020-01003-z Thrombocytopenia and thrombosis in hospitalized patients with COVID-19 https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(20)30178-4/fulltext Megakaryocytes and platelet-fibrin thrombi characterize multi-organ thrombosis at autopsy in COVID-19: A case series https://thorax.bmj.com/content/76/4/412 COVID-19, immunothrombosis and venous thromboembolism: biological mechanisms
We could go on and on… This article explains so much: https://particleandfibretoxicology.biomedcentral.com/articles/10.1186/s12989-016-0168-y Toxicity of graphene-family nanoparticles: a general review of the origins and mechanisms | Particle and Fibre Toxicology | Full Text (biomedcentral.com)
Thank you, greatly appreciated!
It is urgent to stop:
The 2023 digital dollar (Federal Reserve is testing it): they plan to ban cash. We need a law forbidding banning cash. Also, a zero inflation new coin backed by real assets (gold, silver, copper, lithium, oil, soya warrants, whatever but real, since freemasons counterfeit dollars and Euros as explained by Ronald Bernard).
The 2024 WHO International Pandemic Treaty: they plan nations to give up their sovereignty to the WHO
https://scientificprogress.substack.com/p/the-threat-of-the-international-plandemic
The 2025 new plandemic: 67 P4 labs like Wuhan are working in new Frankensteins, we need a REAL non-proliferation Bioweapons Convention.
https://scientificprogress.substack.com/p/the-real-covid-timeline
The 2026 global drought through cloud dissolving tech: we need an international anti-geoengineering Convention.
And this law is also urgent:
So what's really more urgent is a law stating under severe penalty for non-compliance (even to their heirs if that is known after they died), that anyone should disclose if they belong to a secret society, especially those with the requirement to obey secret orders, such as all lodges and freemasonic and luciferian/satanic type of societies.
Penalties should be even more severe with all stake holders involved in or with all the 3 branches of government (even suppliers and candidates), finance (especially, banks, funds, listed corporations) and especially, the armed forces, even the police (that's the reason they' didn't protect the country against blatant constitutional violations).
If this law passes, you'd learn that all listed financial and corporate boards are controlled by freemasons, all the Democrats and especially all the Republicans voting for gender ideology were freemasons, all politicians members of the CFR or attending Sun Valley are freemasons, most of the Supreme Court and lesser courts, all dominant media CEOs are freemasons.
Only then people will ask for change, for example, a law barring them from all such positions. There's no deep state just freemasonry. There are no conspiracies, just freemason plots. There's no democracy with freemasonry, only conspiracy. There’s no 2030 globalism without freemasonry. Freemasonry is the enemy of the people.
Finally, warn him about THE complete plan:
https://scientificprogress.substack.com/p/the-plan-revealed
and the the new plandemic, decarbonization:
https://scientificprogress.substack.com/p/killing-me-softly-with-green-songs