

ROBERT W MALONE: Vaccines “on demand”

ROBERT MALONE: The father of WARP-SPEED? (a specific concept, namely the idea of faster-than-light, or as J. Small of Pfizer puts it, "SPEED OF SCIENCE" VACCINE)


The design process—from genome to gene sequence, ready to insert in a DNA plasmid—can now be accomplished in less than 24 h. While these vaccines are by no means “standard,” the need for innovation in the vaccine design and production process is great. Should such vaccines be developed, their 60-d start-to-finish timeline would represent a 2-fold faster response than the current standard.
Members of the FastVax consortium are well aware that there are many obstacles to overcome before the proposed “rapid response” or FastVax platform for biodefense vaccines can be implemented. Nonetheless, there is a critical national need for an accelerated vaccine design, development and production process that can be accomplished in weeks, not months, in the event of a serious infectious disease outbreak or biowarfare attack. The development of a rapid response to emerging infectious disease threats, using best in-class technologies to provide a first line of defense, will contribute to greater biodefense preparedness and a significant improvement in the ability of the US to protect its citizens against pandemic infectious diseases. The need for new vaccines for protecting against bioterror pathogens and emerging infectious disease is great, and we would argue that, for the reasons cited above, the time to advance these vaccines to the clinic is now.
https://vaccines.unitedscientificgroup.org/2015/ Vaccines R&D-2015 | November 02-04, 2015 Baltimore, USA | United Scientific Group
http://web.archive.org/web/20171008161505/http://www.atheric.com/team/

"orphan" PHAC/rVSV ZEBOV vaccine:
https://wwwnc.cdc.gov/eid/article/26/3/19-1018_article:
Pregnancy Outcomes among Women Receiving rVSVΔ-ZEBOV-GP Ebola Vaccine during the Sierra Leone Trial to Introduce a Vaccine against Ebola
Abstract
Little information exists regarding Ebola vaccine rVSVΔG-ZEBOV-GP and pregnancy. The Sierra Leone Trial to Introduce a Vaccine against Ebola (STRIVE) randomized participants without blinding to immediate or deferred (18–24 weeks postenrollment) vaccination. Pregnancy was an exclusion criterion, but 84 women were inadvertently vaccinated in early pregnancy or became pregnant <60 days after vaccination or enrollment. Among immediate vaccinated women, 45% (14/31) reported pregnancy loss, compared with 33% (11/33) of unvaccinated women with contemporaneous pregnancies (relative risk 1.35, 95% CI 0.73–2.52). Pregnancy loss was similar among women with higher risk for vaccine viremia (conception before or <14 days after vaccination) (44% [4/9]) and women with lower risk (conception >15 days after vaccination) (45% [10/22]). No congenital anomalies were detected among 44 live-born infants examined. These data highlight the need for Ebola vaccination decisions to balance the possible risk for an adverse pregnancy outcome with the risk for Ebola exposure.
Results
Of the 8,651 participants enrolled in STRIVE, 3,101 were women of reproductive age (18–49 years of age). Eighty-four (2.7%) of these women had a singleton pregnancy (no multiple gestations) with EDC <60 days from enrollment or vaccination, including 31 in the immediate vaccinated group, 35 in the unvaccinated group, and 18 in the deferred crossover vaccinated group. At enrollment, the median age of these women was 28 years (range 20–40 years); most of these women were nurses (66 [79%]) or frontline Ebola responders (14 [16%]) (Table 1). Baseline demographic characteristics of vaccinated (immediate and deferred crossover) and unvaccinated pregnant women were generally similar.
The 84 pregnancies led to 51 live births (49 term and 2 preterm) and 30 pregnancy losses (Table 1). For 3 women (2 unvaccinated and 1 deferred crossover vaccinated), the pregnancy outcome was not known. No ectopic pregnancies or neonatal deaths were reported. Of the 51 live births, 29 were in vaccinated women and 22 in unvaccinated women. Most (46 [90%]) infants were delivered in a hospital; 5 (10%) were born at home. The median birth weight was 3,210 g (range 2,400–5,200 g). STRIVE staff obtained consent to examine 44 of the 51 infants (born to 28 vaccinated and 16 unvaccinated women); no external congenital anomalies were documented among these infants.
A total of 7 serious adverse events (SAEs) were reported among pregnant participants. Five SAEs were hospitalizations for a pregnancy-related complication: gestational hypertension (2 cases), prolonged labor (2 cases), and a postpartum hemorrhage (1 case) that resulted in a maternal death. Two pregnant women had hospitalizations for SAEs not related to pregnancy (1 for enteritis and 1 for malaria).
The few published data on pregnancy loss for Sierra Leone are limited to stillbirths (late pregnancy) (22) and do not include spontaneous or induced abortions. However, some conditions common in Sierra Leone, such as malaria, increase the risk for stillbirth and spontaneous abortion (23,24). A limitation of our data is that we were not able to ascertain the number of pregnancy losses in STRIVE that were caused by induced abortion. Induced abortions are illegal in Sierra Leone, but they occur (12). When induced abortions are included in analysis of US pregnancy outcomes, ≈34% of pregnancies end in loss, similar to the loss percentage observed during the STRIVE trial (37%) (25). Because the trial was unblinded, women in the immediate vaccinated group and the unvaccinated group knew their vaccination status, which could have affected their decision-making. For instance, vaccinated women might have been concerned about the safety of the vaccine in pregnancy and thus were more likely than unvaccinated women to terminate the pregnancy, and unvaccinated women might have been more likely to terminate in the context of the outbreak. Also, STRIVE was launched during a terrible epidemic that caused enormous social upheaval. This timing might also have affected decision-making about pregnancy termination.
“Because the trial was unblinded, women in the immediate vaccinated group and the unvaccinated group knew their vaccination status….”
My simple question is:
With the nanotechnology being used in Hospira and Baxter's saline solution - DO WE HAVE A PLACEBO GROUP AT ALL?
Or are ALL these pregnancies lost due to the toxicity of the nanotechnology/graphene in these injections?
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2816%2932621-6/fulltext Efficacy and effectiveness of an rVSV-vectored vaccine in preventing Ebola virus disease: final results from the Guinea ring vaccination, open-label, cluster-randomised trial (Ebola Ça Suffit!)

80 serious adverse events were reported. The most common diagnosis was Ebola virus disease in 39/80 participants (48·7%) followed by road traffic accident injury in 4/80 (5%; appendix). Two serious adverse events were judged to be related to vaccination (a febrile reaction and one anaphylaxis, which resolved without sequelae) and one possibly related (influenza-like illness) which also recovered without sequelae. 15 serious adverse events occurred among enrolled but non-vaccinated participants; 14 were Ebola virus disease in participants (all with onset 0–10 days after randomisation) and one was a road traffic accident injury.
The most common systemic adverse events were headache (46·8% [22 of 47] vs 27·7% [26 of 94]), fatigue (38·3% [18 of 47] vs 19·1% [18 of 94]), myalgia (34·0% [16 of 47] vs 10·6% [10 of 94]), subjective fever (29·8% [14 of 47] vs 2·1% [two of 94]), shivering or chills (27·7% [13 of 47] vs 7·4% [seven of 94]), sweats (23·4% [11 of 47] vs 3·2% [three of 94]), joint aches and pain (19·1% [nine of 47] vs 7·4% [seven of 94]), objective fever (14·9% [seven of 47] vs 1·1% [one of 94]), and joint tenderness or swelling (14·9% [seven of 47] vs 2·1% [two of 94]), arthritis 4·5% (19 of 418). Post-vaccination dermatitis occurred in 5·7% (24 of 418) of vaccinees. A low-level, transient, dose-dependent viraemia occurred in concert with early reactogenicity.
https://www.cdc.gov/vhf/ebola/clinicians/vaccine/precautions.html
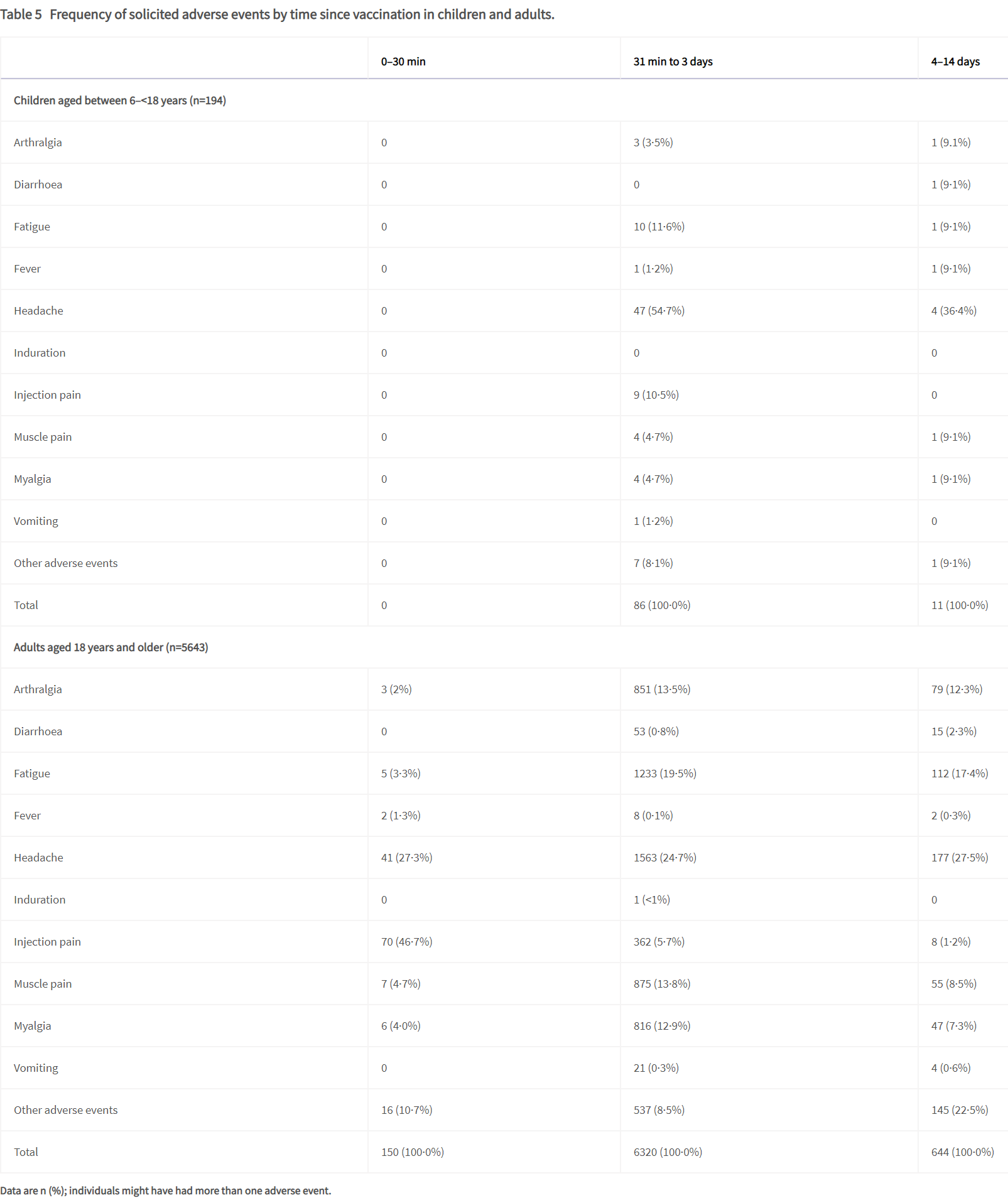
Vaccine adverse events
The most commonly reported injection site adverse events among the adults vaccinated with rVSVΔG-ZEBOV-GP during clinical trials were injection site pain (70%), swelling (17%), and redness (12%). The most commonly reported systemic adverse events following vaccination with rVSVΔG-ZEBOV-GP were headache (37%), feverishness (34%), muscle pain (33%), fatigue (19%), joint pain (18%), nausea (8%), arthritis (5%), rash (4%) and abnormal sweating (3%).
The potential for previously not known, rare, serious events following vaccination may be possible. Administering healthcare providers should monitor individuals for signs and symptoms of reactions following vaccination. Appropriate medical treatment and supervision must be available in case of an anaphylactic event.
Some vaccinated individuals may experience arthralgia and arthritis after vaccination.
However, some vaccinated individuals reported prolonged and recurrent arthritis symptoms. One post hoc analysis identified women and individuals with a medical history of arthritis to have a 2.2–2.8 times higher risk of developing post-vaccination arthritis.
Limitations of vaccine effectiveness
The onset of protection and the duration of protection against EBOV following vaccination with ERVEBO is unknown and may not protect all individuals.
http://web.archive.org/web/20171008161505/http://www.atheric.com/team/ Atheric Pharmaceutical LLC (archive.org)
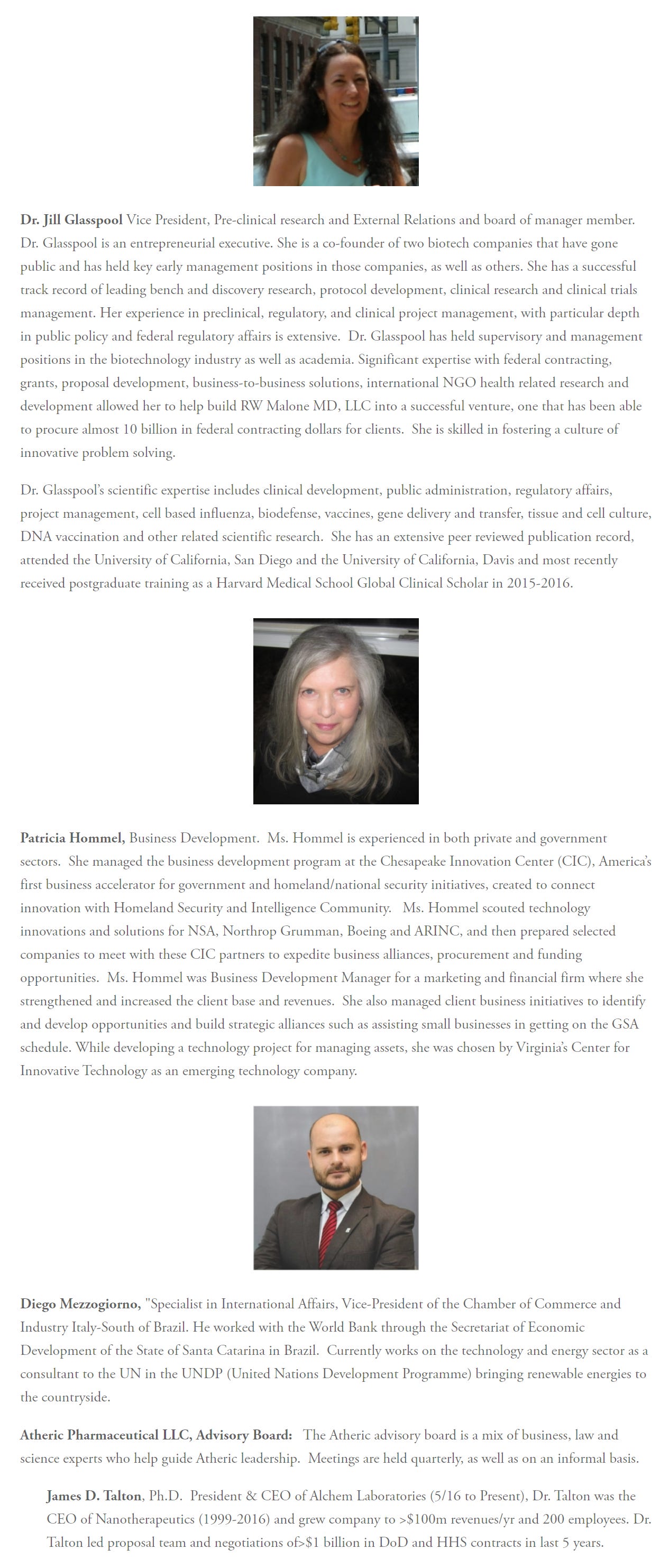
“Currently works on the technology and energy sector as a consultant to the UN in the UNDP (United Nations Development Programme) bringing renewable energies to the countryside.”
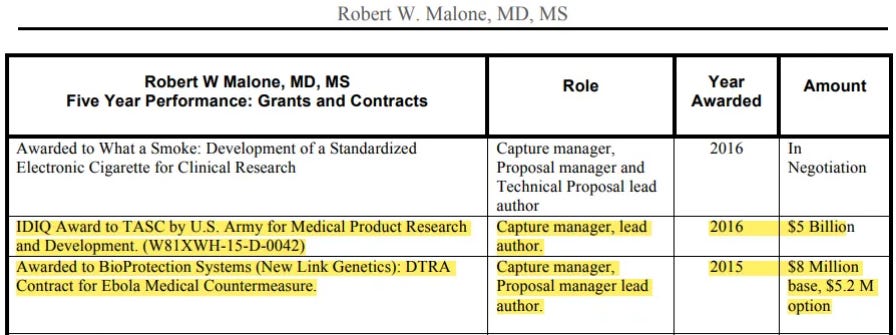
So, does it take 8-10-14 years and more to develop injections for Ebola/Zika/Marburg - or does it take 12 months or even 24 hours?
http://web.archive.org/web/20171008161414/http://www.atheric.com/new-page-3/ Atheric Pharmaceutical LLC (archive.org)
Why Not a Vaccine for Zika?
Vaccines are a great choice for many infectious diseases, but vaccines are time consuming to develop and pose safety risks for some types of infections, including a Zika virus infection.
A recent report by the National Center for Biotechnology Information (NCBI) at the National Institutes of Health estimates that an extremely accelerated pathway for vaccine approval is 8-10 years. For example the West Nile Vaccine (that the Director of National Institute of Allergy and Infectious Diseases (NIAID) promised the US Congress in 2002 would be ready within three years) is just finishing up phase I clinical trials 14 years later.
Infectious diseases, such as the Zika virus, that have a high rate of Guillain-Barré Syndrome (GBS) are generally not good candidates for a vaccine, as the vaccine potentially can also cause GBS. GBS causes a severe form of paralysis and is considered a serious adverse event.
Pregnant women, infants and children are usually excluded from initial vaccine clinical trials, due to safety risks and are usually excluded from new vaccine development, due to unknown risks. A vaccine for Zika would not be initially approved for use in pregnant women and other at-risk populations, such as children and the elderly.
Antibody Dependent Enhancement (ADE) of either Zika or Dengue is a risk with a Zika Vaccine. Testing for this risk is going to be time consuming and costly.
https://finance.yahoo.com/news/soligenix-inc-vital-vaccine-development-165421943.html?guccounter=1&guce_referrer=aHR0cHM6Ly9kdWNrZHVja2dvLmNvbS8&guce_referrer_sig=AQAAAFgGVTnS2Po90-EvG7_oGXnLdfGsdrdFyRMYuFy3ExFXfwyAs0yRw6RmnI47a7bzW6Y1DUVSd0_D4h4nC1IfiknYR1cJRPCm7oswtkKQwCRvBj1hYhVCOdZrzhKOIYiZLtRkW03Kvw6eJtjPzK4Qt79zvyqvzXQdSfOilsbftlFZ Soligenix, Inc: Vital Vaccine Development Program has Potential to Address Future Marburg Virus Outbreaks (yahoo.com)
Soligenix is working to make thermostabilized vaccines a reality, with its ThermoVax(R) platform.
This submission supports a potential multi-year, multi-million dollar contract to develop SuVax(TM) and MarVax(TM) vaccine candidates as medical countermeasures (MCM) for use in the event of a Sudan ebolavirus or Marburg marburgvirus outbreak.
https://www.prnewswire.com/news-releases/soligenix-announces-publication-demonstrating-enduring-protection-of-its-thermostable-rivax-vaccine-301416370.html Soligenix Announces Publication Demonstrating Enduring Protection of its Thermostable RiVax® Vaccine (prnewswire.com)

There is a group guarding the nanotechnology/graphene subject.
WE ARE INJECTED WITH THIS POISON AND WE ARE POISONED BY THIS POISON IN OTHER WAYS!
We, our friends, family members, colleagues, neighbors etc. are injured and die because of this poison!
All while these other people are talking about VIRUSES! in order to divert people's attention away from the REAL PROBLEM AND SOLUTION.
Instead, they offer the Wuhan circus in Congress and the European Parliament, in the media and at conferences.
They take pictures of themselves with the victims and publish their stories to push this f.n agenda. It is beyond comprehension!
It's time to put an end to it and to conduct REAL INVESTIGATIONS!
The lipid nanotechnology Malone invented allows chemicals to pass through the blood brain barrier. He knew this yet he failed to warn the world of the dangers. He watched as the CDC and Fauci claimed the vaccine stayed in your arm yet waited silently in the background. He blames government lack of transparency; how about his lack of transparency? https://www.foxnews.com/media/tucker-carlson-mrna-vaccine-inventor