

STOP DICKING US AROUND

18 U.S. Code § 1038 - False information and hoaxes
(a)Criminal Violation.—
(1)In general.—Whoever engages in any conduct with intent to convey false or misleading information under circumstances where such information may reasonably be believed and where such information indicates that an activity has taken, is taking, or will take place that would constitute a violation of chapter 2, 10, 11B, 39, 40, 44, 111, or 113B of this title, section 236 of the Atomic Energy Act of 1954 (42 U.S.C. 2284), or section 46502, the second sentence of section 46504, section 46505(b)(3) or (c), section 46506 if homicide or attempted homicide is involved, or section 60123(b) of title 49, shall—(A)be fined under this title or imprisoned not more than 5 years, or both;(B)if serious bodily injury results, be fined under this title or imprisoned not more than 20 years, or both; and(C)if death results, be fined under this title or imprisoned for any number of years up to life, or both.
So now we have so many deaths and injuries and yes, we have all been lied to. The so-called Covid is caused by nanotechnology used in flu vaccines, masks, PCR tests, food and in many other ways - but it has been used "for your benefit." It is the cause of acute oxidative stress, especially in the more vulnerable. Acute oxidative stress causes cell death, blood clots, organ failure, low saturation, strokes, heart failure, etc. Graphene causes ARDS - acute respiratory distress syndrome. Graphene nanotechnology crosses blood barriers and its toxicity causes known Covid symptoms.
THIS NEEDS TO BE INVESTIGATED!!!
So why do Ivermectin and NAC and many other supplements and drugs work? Because they have antioxidant properties or are antioxidants. THIS IS THE CURE FOR THE DISEASE.
It is demonstrated here:
In recent decades, knowledge regarding oxygen free radicals (OFRs) has generated a lot of interest due to the role that these molecules play in various clinical situations encountered in medical practice. Tissue damage caused by OFRs is seen in various conditions, such as clinical shock, septicemia, systemic inflammatory response, fulminant hepatitis, alcoholic hepatitis, organ transplant, cardiac failure, respiratory failure, etc. What all of these clinical situations have in common is either hypoxic microenvironments followed by reoxygenation or ischemic microenvironments followed by reperfusion. Both conditions facilitate OFR generation.
Systems of defense against oxidative aggression
The antioxidant defense system is composed of the suite of substances that neutralize the hazardous effects of OFRs. Enzymes found in the cytosol, such as SOD, catalase, and glutathione peroxidase, have also been observed in mitochondria, where a great number of OFRs are produced.
Recently, Davies proposed a comprehensive classification of the antioxidant defense system, divided into primary and secondary defense. Primary defense includes antioxidant complexes such as vitamins (E, A and C), glutathione, uric acid, and antioxidant scavenger enzymes (such as SOD, catalase and the peroxidases). Secondary defense includes lipolytic enzymes, phospholipases, proteolytic enzymes, DNA repair enzymes, endonucleases, exonucleases, and ligases.
The reduced form of the tripeptide glutathione (gamma-glutamyl-cysteinyl-glycine) is the most abundant low-molecular-weight thiol in virtually all mammalian cell systems. The chemical versatility of reduced glutathione, especially its interaction with various oxidant components such as *O2-, H2O2, and *OH, makes it an efficient reductant. Reduced glutathione is found in high concentrations in bronchoalveolar lavage fluid, conferring protection against oxidative injury to the lungs. The importance of reduced glutathione was confirmed in studies in which its depletion was related to a higher risk of pulmonary disease.
N-acetylcysteine is a mucolytic drug and has antioxidant properties since it is a precursor of reduced glutathione.
NAC (N-acetylcysteine) is a precursor of glutathione! Higher doses would help against Covid and also injuries the toxicity of those injections cause!!!
So, what happens when you inhale it and WHY IS THIS IN ALL MASKS and PCR TESTS?
Findings from several recent studies indicate that graphene and graphene oxide (GO) may induce the acute inflammation and pulmonary fibrosis in mice lungs. Nanoparticles may translocate to extrapulmonary organs and may be redistributed to other tissues after deposition in the lung. Thus, knowledge of graphene biodistribution in mice after inhalation remains a key research gap. FLG may pass through the air-blood barrier into blood and then be delivered to liver and spleen, or enter into the blood via adsorption through the gastrointestinal tract.
When considering the potential human health risks of nanoparticles, inhalation is thought to be the exposure route of highest concern.
https://www.nature.com/articles/am20137#MOESM2
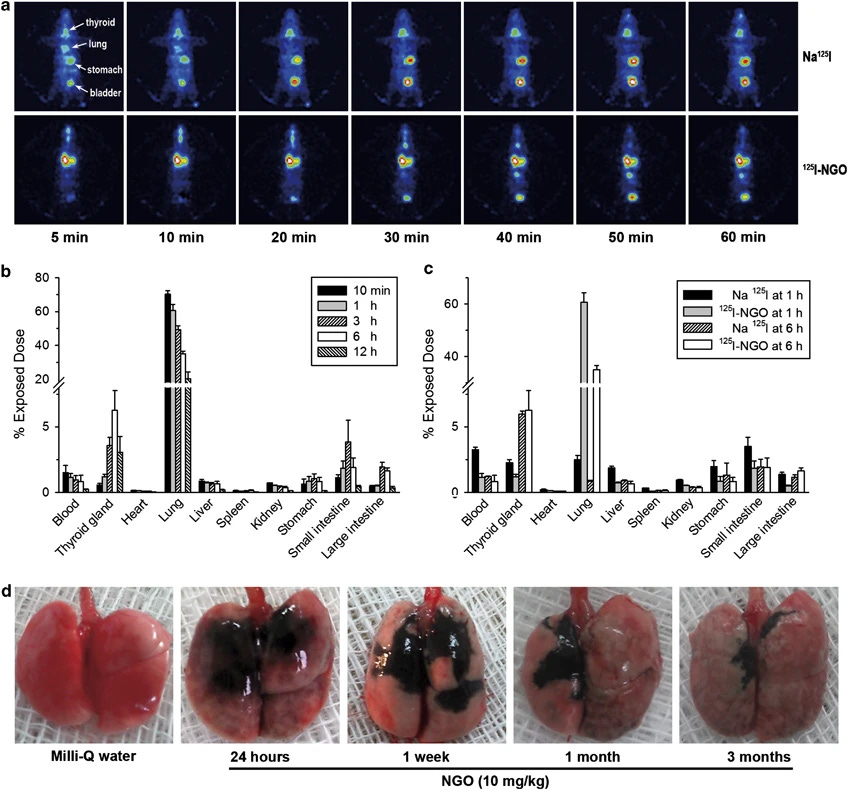
Biodistribution of NGO (nanoscale graphene oxide) after intratracheal instillation. (a) SPECT images of mice at several time points after intratracheal instillation with 125I-NGO or Na125I. (b) Distribution of 125I-NGO in the blood and major organs of mice at five different time points. N=5 in each group. Values are presented as the mean±s.e.m. (c) Comparison of Na125I and 125I-NGO distribution in mice at 1 and 6 h after intratracheal instillation. N=5 in each group. Values are presented as the mean±s.e.m. (d) The morphological observation of the lungs from mice instilled with Milli-Q water or 10 mg kg−1 NGO. The dorsal view shows the distribution of NGO (black region).
CELL INJURY IN THE LUNG IS OFTEN ASSOCIATED WITH LUNG EDEMA, WHICH IS THE RESULT OF THE LEAKAGE OF FLUID FROM THE CAPILLARIES INTO THE INTERSTITIAL AND ALVEOLAR SPACES AND THE LOSS OF THE LUNG’S ABILITY TO PUMP FLUID OUT OF THE AIRSPACE. INDEED, WE FOUND THAT NGO (nanoscale graphene oxide) LED TO AN INCREASE IN THE LUNG WET/DRY WEIGHT RATIO IN A DOSAGE-DEPENDENT MANNER; THIS RATIO IS AN INDICATOR OF THE SEVERITY OF THE LUNG EDEMA.
Given that NGO (nanoscale graphene oxide) caused ALI (Acute Lung Injury) at 24 h post exposure, we examined the time-dependent pulmonary responses induced by NGO. LDH and ALP activities were elevated at 24 h and then decreased, suggesting that NGO induces early severe cell damage. The peaks of BAL fluid total protein, lung wet/dry weight ratio and BAL fluid differential cell counts occurred at 48 h, suggesting that this is the time point of the most severe disruption of the alveolar–capillary interface, lung edema and neutrophil infiltration
Moreover, the diffuse lung edema with protein-rich fluid, extensive hemorrhage and significant changes in alveolar architecture were clearly observed 48 h after instillation
Considering the wide distribution range of graphene sizes in our study, a fraction of graphene likely passed the air-blood barrier and was translocated to liver and spleen. Li et al applied 125I labeled GO to study its distribution in Kunming mice by intratracheal instillation and found that the radioactivity was detected in blood and organs, including liver, spleen and thyroid gland.
Because the inflammatory responses caused by nanomaterials are often associated with oxidative stress, we examined the degree of oxidative stress in the lung by measuring the levels of two antioxidants, superoxide dismutase (SOD) and glutathione peroxidase (GSH-PX). We observed a dosage-dependent decrease in SOD and GSH-PX activities in the lung tissue. In addition, the SOD and GSH-PX activities were progressively reduced after the exposure to NGO, reaching a minimum at 48 h, followed by an elevation until 1 week. These data suggest that oxidative stress has a significant role in NGO-induced ALI. NGO was still present in the lung at 3 months. NGO caused dosage-dependent ALI characterized mainly by cell injury, lung edema and neutrophil infiltration. The NGO-induced ALI was progressive, as it was most severe at 48 h and was then alleviated. The NGO-induced chronic pulmonary lesions were characterized by diffuse pulmonary fibrosis. The NGO-induced ALI was related to oxidative stress and could effectively be relieved with DEX treatment. The fact that inhaled NGO is harmful to animals might raise environmental concerns, particularly under the context that radioactive species may be carried by these carbon nanomaterials. Nanoscale, ultrafine particulates (<100 nm in diameter) from natural and anthropogenic sources have become the cause of rapidly increasing concern. Severe adverse health effects of inhalable ultrafine particulate matter have been demonstrated in both pulmonary toxicity and epidemiological studies. There is a body of evidence that particulate matter can penetrate deeply into lung tissue with larger numbers and stay longer than fine or coarse particles (micrometer size or larger). Because of their small sizes and high ratios of surface area to mass, carbon-based nanoparticulates are highly adsorptive to toxic substances, including radioactive species, which has attracted significant recent concern. Given that the biodistribution of 125I-NGO varies greatly from that of 125I ions, it is possible that nanoparticulates can deliver radioactive isotopes deep into the lungs. These nanocarriers may also alter the biodistribution of the radioactive isotopes, settling in numerous ‘hot spots’ that can result in mutations and cancers. Although studies of such potential risks of radioactive nanoparticulates are still rare, THE DATA REPORTED HERE HIGHLIGHT THE SIGNIFICANCE OF PROTECTIVE STRATEGIES TO MINIMIZE HUMAN EXPOSURE TO NGO SOURCES. In addition, the possibility to reduce the NGO-induced toxicity by optimization of its sizes and surface coatings should be explored in future studies
Nowadays, with the development of methodologies based on oxidation-sensitive proteins, it is known that ROS and oxidative damage increase in hypoxia.
The generation of hypoxia occurs when staying at high-altitude environments or when receiving mixtures of contaminated gases.
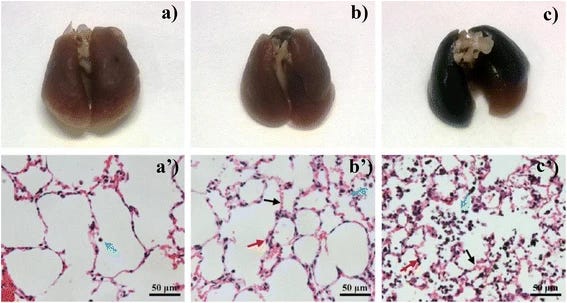
The morphological observation and representative H&E stained images of the lungs harvested 24 h post exposure (a and a’ control group; b and b’, 5 μg exposed dose; c and c’, 50 μg exposed dose). Sections were analyzed blindly and representative images selected from 6 mice per treatment group are shown. Blue arrows: cells in alveoli; red arrows: parenchymal; black arrows: interstitial edema
To explore the time-dependent toxicity of graphene after intratracheal instillation, H&E and Masson staining were applied to examine pathological changes of lung tissue. As shown when control Fig. 6 (a) is compared to Fig. 6 (b), moderate interstitial and parenchymal edema was observed in H&E stained lung sections after exposure for 1 day. Severe inflammatory cell infiltration were also observed, which was characterized by substantial quantities of cells in the pulmonary alveoli. Though the severity was reduced, minimal pulmonary edema and inflammatory infiltration was also observed after 7 days.
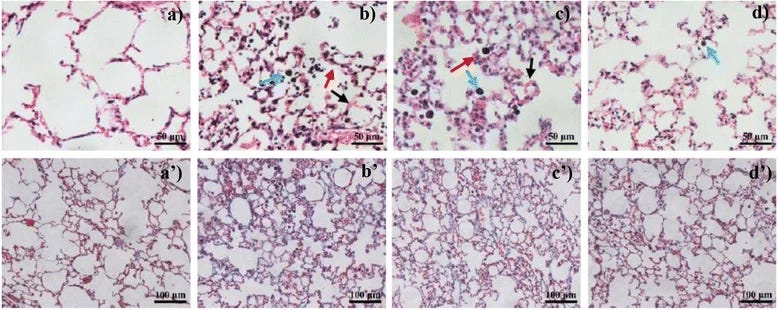
H&E (a, b, c, d) and Masson (a’, b’, c’, d’) stained lung sections of mice which were exposed 50 μg FLG at different time points post exposure (a and a’ were control group at 1 day post exposure; b and b’ were 1 day post exposure; c and c’ were 7 days post exposure; d and d’ were 28 days post exposure). Sections were analyzed blindly and representative images selected from 6 mice per treatment group are shown. Blue arrows: cells in alveoli; red arrows: parenchymal; black arrows: interstitial edema
Indeed, a recent study on mice demonstrated that intratracheally delivered few-layered graphene was mainly retained in the lung, with 47% remaining after 4 weeks and this resulted dose-dependent acute lung injury and pulmonary oedema.
Effects of GO on Important Organs
We also investigated the effects of GO on organs of mice. We learn from the pathology and light micrograph that the GO accumulations were primarily in the lungs, liver, and spleen. There were obvious chronic toxicity responses occurring in the lungs and liver after tail vein injection. Histopathological analysis revealed that pulmonary exposures to GO produced a dose-dependent lung inflammatory response characterized by neutrophils and foamy alveolar macrophage accumulation.
The treated mice exhibited a dose-dependent series of granulomas. With the increase in GO dose, the toxicity reaction of the lung of mice becomes more and more severe. For example, GO induced dose-dependent epithelioid granulomas and, in some cases, interstitial inflammation in the mice. Large amount of inflammation cells was infiltrated in lung alveolus interstitium; the alveolar septa became thicker and some lung alveoli were cracked.
Lung damage is the chief human toxicity concern surrounding nanotechnology, with studies showing that most nanoparticles migrate to the lungs. However, there are also worries over the potential for damage to other organs.
For example, studies have established that the comparatively large surface area of inhaled nanoparticles can increase their toxicity. Such small particles can penetrate deep into the lungs and may move to other parts of the body, including the liver and brain.
As hazardous as asbestos? A major study published in Nature Nanotechnology in May 2008 suggested some forms of carbon nanotubes could be as harmful as asbestos if inhaled in sufficient quantities.
Nanoparticles can get into the body through the skin, lungs and digestive system. This may help create 'free radicals' which can cause cell damage and damage to the DNA. There is also concern that once nanoparticles are in the bloodstream they will be able to cross the blood-brain barrier. 3.The human body has developed a tolerance to most naturally occurring elements and molecules that it has contact with. It has no natural immunity to new substances and is more likely to find them toxic. The danger of contact with nanoparticles is not just speculation. As more research is undertaken, concerns increase. Here are some of the recent findings: • some nanoparticles cause lung damage in rats. Several studies have shown that carbon nanotubes, which are similar in shape to asbestos fibers, cause mesothelioma in the lungs of rats • other nanoparticles have been shown to lead to brain damage in fish and dogs • a German study found clear evidence that if discrete nanometer diameter particles were deposited in the nasal region (in rodents in this case), they completely circumvented the blood/brain barrier, and travelled up the olfactory nerves straight into the brain • inhaled carbon nanotubes can suppress the immune system by affecting the function of T cells, a type of white blood cell that organizes the immune system to fight infections.
https://www.chemistryworld.com/news/graphene-slips-deeper-into-lungs-than-predicted/3001864.article
Researchers discover that once graphene enters the lungs the immune system has trouble getting rid of it. Graphene nanoplatelets can penetrate deeper into the lungs than their size would suggest, say UK researchers. And once there, the body’s natural defences cannot deal with them effectively. Chronic exposure could therefore lead to inflammation and disease in a similar way to asbestos fibres.
Can graphene take part in the fight against COVID-19? (nih.gov) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7203038/
Limitations and Challenges Even if the antiviral efficacy of graphene has been demonstrated, the immediate use of graphene for treatment of COVID-19 is unrealistic. The only available in vivo test for virus treatment demonstrated the efficacy of GO-hypericin in ducklings infected with the Novel duck reovirus. We should however point out that in vivo toxicity of graphene is still a matter of debate. Graphene materials can cross biological barriers but are less cytotoxic toward macrophages, important cells for immunological response, compared with other carbon nanomaterials. Conclusions on graphene toxicity are however made difficult due to the infinite combinations of dose, surface chemistry, exposure route used for the evaluation. Its instability and aggregation in solution are further problems, given the mandatory stability required for drugs and vaccine storage prior use.
And they dare to call it disinformation!
This is a crime, it needs to stop, and it needs to be investigated, and criminal charges should be filed!
It dosen't need to stop and doesnt need to be investigated, because nobody wants it to. They don't want it to because they don't know the risks, and have been taught it's their only salvation. Most people still believe covid has 20 or 30 % mortality among the unvaxed. They don't know the truth because they've been lied to by politicians, doctors and journalists, and because they're stupid.
We need to focus on educating the public on the risks, so they'll demand honest treatment. That will, in turn, require the politicians, doctors, and journalists to stop misbehaving and begin investigating the problems, and deveop real solutions.
Kirsch is starting to use billboards. Media is becoming more receptive to the truth, and will accelerate after tuesday's election, lest they make primetime news in the hot seat of congressional inquisitors. Articles and ads will proliferate. We're on the verge of recovery, but it's important to keep the pressure on, calmly and unemotionally. Outrage won't help. It was useful initially, but now it's becoming a standard marketing problem. That's priority 1 -- making it stop.
Priority 2 is to deliver justice to the perpetrators of millions of unnecessary deaths, incalculable suffering, and trillions in finanial losses. Outrage can still be useful for that.
Thanks. Reading it again. So outraged!